55 year old female with Uncontrolled Glucose levels.
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
A 55 year old female , daily labourer by occupation resident of Suryapet came for insulin dose fixation for eye surgery.She is a known case of Diabetes.
HISTORY OF PRESENTING ILLNESS
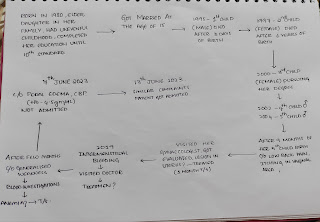
Patient was apparently asymptomatic 2 years ago. On one fine day while she was doing her household work she had giddiness which lasted for a while and has been taken to a nearby hospital ,blood and urine investigations were done.She gave a history of increased frequency of urine since 1month.
No H/o nocturia , burning micturition.
H/o generalised weakness since 15 days .
H/o increased thirst (polydipsia) since 1 week .
H/o vomitings 4 days ago (3 times/ day ) food as content,non projectile in nature,non blood stained .
No h/o loose stools,blood in stools.
No h/o fever ,rash, abdominal pain.
No h/o palpitations, sweating.
2 years ago she was diagnosed with diabetes mellitus at the near by hospital and was on medication since then.(Tab .Metformin 500 mg
On the date of admission,
Diminishing of vision since 6 months in the left eye and was posted for surgery ,but her glucose levels were abnormal so referred for control of glucose levels to bring down to normal levels .
No H/o loss of sensation in limbs.(upper and lower)
No H/o tingling sensation in limbs.
No H/o swelling in ankles ,feet, hands and legs.
PAST HISTORY
Diabetes Mellitus since 2 years.(on medication)
No H/o Hypertension, Tuberculosis,Asthma, Thyroid disorders
PERSONAL HISTORY
Appetite-Normal
Diet-Mixed diet
Bowel and Bladder movements- Regular
No H/o allergies
No addictions
FAMILY HISTORY
Elder brother is a known case of Diabetes
TREATMENT HISTORY
Metformin -500mg BD
Inj.Mixtard 20U M,20 UN ( 2times /day)
GENERAL EXAMINATION
On examination, patient is conscious, coherent, cooperative
Patient is moderately nourished
No pallor,icterus, cyanosis, clubbing, lymphadenopathy, edema
Vitals
Temperature- afebrile
Pulse rate -79/min
Respiration rate-18/min
BP-110/70mm/Hg
SYSTEMIC EXAMINATION
Cardio vascular examination:
No visible pulsations, scars, engorged veins. No rise in jvp
Apex beat is felt at 5 Intercoastal space medial to mid clavicular line.
S1 S2 heard . No murmurs.
Respiratory system
Shape of chest is elliptical, b/l symmetrical.
Trachea is central. Expansion of chest is symmetrical
Bilateral Airway Entry - positive
Normal vesicular breath sounds heard
CNS EXAMINATION:
No signs of meningeal signs
Cranial nerves: normal
Sensory system: normal
Motor system: normal
Reflexes: Right. Left.
Biceps. ++. ++
Triceps. ++. ++
Supinator ++. ++
Knee. ++. ++
Ankle ++. ++
Gait: normal.


On 9/11/2021
Ophthalmology referral

Investigations
1.GRBS charting regularly
Before breakfast
After breakfast
Before lunch
After lunch
Before dinner
After dinner.

PROVISIONAL DIAGNOSIS
Uncontrolled glucose levels.
TREATMENT
1.GRBS charting regularly.
2.Inj.Human insulin s/c
NPH -10 U (twice daily)
3.check for symptoms of hypoglycemia
4.Inj .25 D if GRBS shows <50mg/dl.

Comments
Post a Comment