25 year old female with bloody loose stools and pain during defecation.
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
CASE
A 25 year old female tutor by occupation came from West bengal to OPD with chief complaints of bloody loose stools and pain during defecation since 4 months.
HISTORY
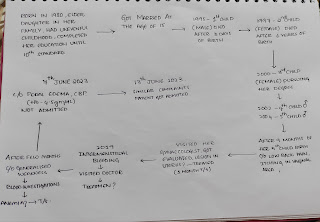
Patient was apparently asymptomatic 4 months ago.Then she started having bloody loose stools (4-5times perday) .she consulted a physician who prescribed her few medication but they didn't work.So ,she consulted same doc once again who said itcould be because of infection and prescribed her medicine.Then her stools became hard and painful to defecate.so she stopped thos e medicines on her own.Then in the end of April she consulted another Doctor who sent her for few lab investigations like colonoscopy, USG .On colonoscopy they found out that there is an ulcerated lesion (5cm ) at the anal leverage.In USG they found out that there is Rt renal calculus (3.4mm).Then she was on medication.After taking medication she has recovered from bloody loose stools.But,it didn't subside completely.So,Later she consulted another physician when her frequency of micturition increased (5-6times /day) with an incomplete post voidal feeling.There,she was treated with T.Zanocin OZ and T.Rifagut TD.
She has also complaint of pain in the left iliacand lumbar fossa since 4 months occassionally.
Daily routine:
She is a post graduate student who tutors 2 times per day(morning and evening) and does house hold work .
She wakes up in the morning at 7 am ,have her breakfast leave for tutorial classes .Later in the afternoon she will have her lunch at 2 pm and then again goes to tutorial session for3 hrs in the evening.After this she comes home does some house hold work,have dinner and goes to bed around 11pm.
Personal History
Mixed diet
She was on diet since 2 years to maintain fitness.
She use to eat lot of spicy food during her college days .
Since 2 months she stopped eating spicyfoods and other certain kinds of food on her own accord.
Abnormal Appetite
Bloody loose stools (pain during defecation)
Increased micturition
Adequate sleep
No addictions.
Past History
Nota known case of Diabetes, Hypertension, Asthma, Tuberculosis, Epilepsy.
Family History
Not relevant
Treatment History
T.Rifatgut (TD)
T.Zanocin OZ
General Examination
Patient was conscious, coherent and cooperative.she was well oriented to time place and person.
Vitals
BP:124/80 mmHg
PR:65bpm
RR:16cpm
Temperature: Afebrile.
No pallor
No icterus
No cyanosis
No clubbing
No lymphadenopathy
No Edema.


Systemic Examination
Per Abdomen :
No scars seen
Shape of abdomen– flat

Umbilicus
Position-central , Shape-slit
No tenderness
No organomegaly
Bowel sounds heard
CVS:
S1 S2 Heard,no murmurs heard
Respiratory system:
Normal vesicular sounds heard .
Bilateral airway clear.
CNS:
No neurological deficit found.
Provisional diagnosis:
Inflammatory Bowel Disease.
Investigations:
Posted for colonoscopy on July 8 2022.
Colonoscopy on 20 May 2022


On 20 May 2022


Comments
Post a Comment