45 year old male with Chronic Kidney Disease
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
A 45 year old male security guard by occupation came to OPD with chief complaints of
Shortness of breath since 5 days
Decreased urine output since 5 days
Swelling in both lower limbs since 5 days
HISTORY OF PRESENTING ILLNESS
Patient was apparently asymptomatic 5 days ago.Then he started having breathlessness,insidious in onset , gradually progressive in nature (Grade 2 - Grade 3) aggravated on walking and relieved on sitting.
No H/o orthopnea, paroxysmal nocturnal dyspnea.
H/o decreased urine output since 5 days. associated with increased in frequency in small amounts.
H/o swelling in both limbs below knee since 5 days which was insidious in onset and gradually progressed from ankle upto knee .It relieved on after dialysis.
No H/o nocturia.
No H/o nausea, vomiting, loose stools, constipation.
No H/o fever, cough ,cold .
No H/o palpitations, sweating .
No H/O chest pain.
No H/o abdominal distension, abdominal pain.
No H/o hematuria.
No h/o headache,sleep disturbances.
PAST HISTORY
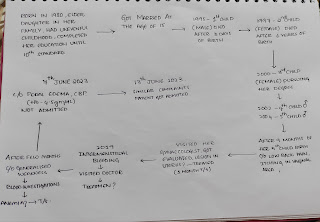
H/ o similar complaints in the past.He had similar complaints 5 years ago.He had bilateral pedal edema and decreased urine output so he came to our OPD and was diagnosed with renal failure after performing investigations.He is maintained on hemodialysis since then (twice weekly)
K/c/o Diabetes and Hypertension (11 years ) .He is on medication.
Not a k/c/o Tuberculosis, Epilepsy, Asthma
PERSONAL HISTORY
Mixed diet
Normal Appetite
Adequate sleep
Regular bowel movements.
Decreased urine output.
No allergies
Occasional alcoholic
No smoking
FAMILY HISTORY
Not relevant
TREATMENT HISTORY
He is maintained on hemodialysis
Last 2 were on April 3 2023 and April 6 2023.
Hypertension: clinidipine 10 mg
GENERAL EXAMINATION
Patient is coherent,conscious and cooperative .
Patient is well nourished.
Pallor present
No icterus, clubbing, cyanosis,lymphadenopathy,edema.(relieved after dialysis).



Vitals
Temperature :99°F
Blood pressure: 150/80 mm Hg
Pulse rate: 78 bpm
Respiratory Rate: 16 cpm
GRBS -161 mg/dl
SYSTEMIC EXAMINATION:
Respiratory system:
Inspection:
No structural abnormalities in nose, no obstruction in nasal airway .
Oral cavity - no crooked teeth
Pigmented patches present on tongue .
No ulcers in mouth.
Trachea appears to be central.
Bilateral symmetrical.Elliptical in shape.
Symmetrical expansion on both sides.
No scars ,sinuses,engorged veins.
Palpation:
No local rise of temperature
No tenderness.
Trachea is central.
Apex beat present in medical to mid clavicular line in 5th intercostal space.
Chest expansion equal on both sides.
Tactile vocal fremitus present on both sides.
Percussion:
Right Left
Supraclavicular Resonant Resonant
Infraclavicular Resonant. Resonant
Mammary Resonant Resonant
Axillary Resonant Resonant
Infra axillary Resonant Resonant
Suprascapular Resonant Resonant
Infrascapular Resonant. Resonant
Interscapular Resonant. Resonant
Auscultation:
Right. Left
Supraclavicular NVBS. NVBS
Infraclavicular. NVBS. NVBS
Mammary NVBS. NVBS
Axillary NVBS. NVBS
Infra axillary. NVBS. NVBS
Suprascapular NVBS. NVBS
Infrascapular NVBS. NVBD
Interscapular NVBS. NVBS
Cardiovascular system:
Inspection-
No raised JVP
The chest wall is bilaterally symmetrical
No dilated veins, scars or sinuses are seen
Apical impulse at 5th intercostal space
Palpation-
Apex beat is felt in the fifth intercostal space, 1 cm medial to the midclavicular line
Percussion -
Right and left borders of the heart are percussed
Auscultation-
S1 and S2 heard, no added thrills and murmurs are heard
Per abdomen:
Shape of abdomen: obese umbilicus-inverted
No scars, sinuses, engorged veins.
No tenderness
No organomegaly.
Bowel sounds not heard
Central nervous system:
Conscious
Normal speech.
No neurological deficit found.
PROVISIONAL DIAGNOSIS
This is case of patient involving renal system probably chronic kidney disease secondary to Hypertension and Diabetes mellitus.
INVESTIGATIONS
Serum iron -53 microgram/dl
Serum creatinine -15.2 mg/dl
Blood urea -154mg/dL



USG report


Comments
Post a Comment