23 year old female with facial periorbital edema and pedal edema.
This is an a online e log book to discuss our patient de-identified health data shared after taking his/her/guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
The patient/ attender was informed the purpose of the information being acquired. An informed consent was taken from patient/ attender and there is omission of information that was requested to be omitt.
A 23 year old female resident of vutikodu farmer by occupation came to OPD with chief complaints :
✓periorbital edema (on and off) since 5 months.
✓Bilateral Pedal edema (on and off) since 5 months.
✓Fatigue since 5 months.
History of presenting Illness:
Patient was apparently asymptomatic 5 months ago.Bilateral Pedal edema which is pitting type since 5 months which was insidious in onset, gradually progressive in nature, aggrevated while working in farm and relieved on medications.
H/o periorbital edema early in the mornings, deceased as the day progresses since 5 months ( on and off)
H/o fatigue since 5 months.
No H/o polyuria , nocturia, burning micturition.
No h/o fever ,rash , abdominal pain, vomiting, diarrhoea, constipation.
No h/o difficulty in breathing, palpitations, sweating,chets pain,chest tightness.
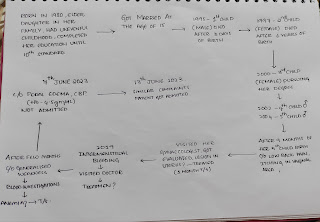
Sequence of events:

Daily routine:
She is a farmer by occupation.She wakes up usually around 5:30 am , sweeps in and around her house, cooks,washes clothes and have breakfast by 9 am and goes to field to work by 10 am .She works in farm for 3 hrs in morning,eats lunch around 1pm and takes rest.She will go home around 6pm after working whole afternoon in the farm , prepares dinner ,eat and sleep around 10 pm .
She farms paddy , cotton and Vegetables in her field.
Past history:
Not a k/c/o Diabetes Mellitus, Hypertension, Tuberculosis, Epilepsy,Asthma, Thyroid disorders.
Personal History:
Diet:mixed
Appetite : normal (generally less appetite)
Bowel is regular
Bladder- decreased urine output(reduced to 1time a day)
Sleep:adequate
No addictions
No allergies
Family History:
No significant family history.
Treatment history:
Inj . DURATAZ 4.5 mg
Tab DYTOR 10 mg
Tab. RABTER D CAP
On presentation her vitals:
BP: 110/90 mm Hg
Respiratory Rate: 20 cpm
Pulse rate: 99 bpm regular,no radio radial delay
SpO2:98% on room air.
GRBS: 83 mg /dL .
Temperature: afebrile
GENERAL EXAMINATION:
patient was conscious,coherent,cooperative.
Moderately built and nourished.
well oriented to time,place and person
No pallor,icterus , clubbing, cyanosis,koilonychia , lymphadenopathy.
B/L pedal edema - pitting type present.





On 30 /11/2022
Vitals
Temperature:Afebrile
BP:130/80 mm of Hg
Pulse rate: 80bpm irregular,normal value.
Respiratory Rate:18cpm
Systemic Examination:
Abdominal examination:
Inspection
Umbilicus inverted , No abdominal distention,no visible pulsations,scars and swelling.
Palpation
Soft, non tender, no organo megaly.
Auscultation
Bowel sounds heard


Cardio vascular examination:
No visible pulsations, scars, engorged veins. No rise in jvp
Apex beat is felt at 5 Intercoastal space medial to mid clavicular line.
S1 S2 heard . No murmurs.
Respiratory system :
Shape of chest is elliptical, b/l symmetrical.
Trachea is central. Expansion of chest is symmetrical
Bilateral Airway Entry - positive
Normal vesicular breath sounds
CNS examination: No neurological deficit found.
Gait: normal.
Normal speech.
Provisional Diagnosis:
Nephrotic syndrome under evaluation.
Investigations:
HEMOGRAM

COMPLETE URINE EXAMINATION

24 HOUR URINE (protein: creatinine)

SERUM CREATININE
SERUM ELECTROLYTE

ECG


Treatment:
1.Salt restriction (<2.4 gm/day)
2.Fluid restriction (<1 lit/day)
3.Tab.Lasix 20 mg PO BD
4.Tab .Ramipril 2.5 mg PO/OD


Comments
Post a Comment