50 Y/M with c/o chest pain and Dyspnoea
A 50 year old male resident of khasanaguda tailor by occupation came with chief complaints
1)chest pain since 3 years
2) shortness of breath since 3 years
3) cough since 1 week
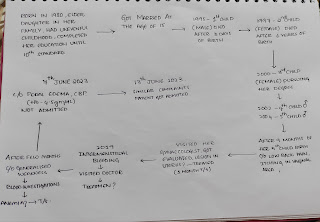
Patient was apparently asymptomatic 5 years ago .
March 2019
He had c/o fever , high-grade , not associated with child and rigors since 4 days , redness , pain and swelling in rt lower limb since 3 days . Initially it started as a bleb and it progressed to swelling of limb associated with pain . He was examined, investigated and diagnosed as Rt lower limb cellulitis with ulcer over rt dorsum of foot.
S/P - Split Skin Graft
Stayed at hospital for 3 months and got discharged



2022
He went to hospital with c/o dyspnea ( grade 2 mmrc ) since 1 month . No h/o chest pain, palpitations, sweating, pedal edema , pnd , orthopnea . He was started on medication
1) T.Aspirin 75 mg
2) T.Atorvastatin 20 mg
3) T.Met xl 15 mg
4) T Lasix 40mg
He was on regular follow up and on regular medication since then .
2023
Patient went with c/o chest pain radiating to the back , left arm since 1 month .
Sob progressed to garde 3 ( MMRC)
H/o fatigue
After investigations were done he was notified his creatinine levels were elevated (?CKD) and underwent 2 sessions of dialysis . Later he was planned for renal biopsy but patient was not willing for it so left the hospital.
From then he is visiting near by government hospital for medication.(monthly)
But from last few months he couldn't afford for the medication and he has stopped taking few of the above mentioned medication.
2024
Patient now complains of chest pain radiating to left upper limb since 3 years aggravating on strenuous exercise and no relieving factors associated with sweating on exertion and not associated with palpitations .
H/o SOB grade 2 MMRC insidious in onset , gradually progressive since 3 years aggravates on exertion and relieves on taking rest .
H/o cough not associated with expectoration since 10 days aggravates during night and no relieving factors.
No h/o orthopnea and paroxysmal nocturnal dyspnea.
No h/o decreased urine output, burning micturition .
No H/o nocturia, polyuria
No H/o nausea, vomiting, loose stools, constipation.
No H/o fever, cold .
No H/o palpitations
No H/o abdominal distension, abdominal pain.
No H/o hematuria.
No h/o headache,sleep disturbances.
N/k/c/o DM, HTN ,TB, Asthma, Epilepsy, Thyroid disorders
Personal History
Appetite - Normal
Bowel and bladder movement - regular
Sleep - adequate
Diet - mixed ( stopped intake of meat since 3 years )
Alcohol consumption since 20 years stopped intake since 3 yrs
Smoker since 25 years (1 pack / day )
Family history:
No significant family history
General physical Examination:
Patient is conscious, coherent and co-operative.
No signs of pallor , icterus , cyanosis , clubbing , clubbing, lymphadenopathy , edema .
Hyperpigmentation seen around the neck


Vitals
BP : 110 / 70 mm hg
PR : 62
RR : 18
Spo2: 95@ RA
Systemic examination:
Cardiovascular system:
Inspection-
No raised JVP
The chest wall is bilaterally symmetrical
No dilated veins, scars or sinuses are seen
Apical impulse at 5th intercostal space
Palpation-
Apex beat is felt in the fifth intercostal space, 1 cm medial to the midclavicular line
Auscultation-
S1 and S2 heard, no added thrills a
nd murmurs are heard
Respiratory system:
Bilateral air entry clear, Normal vesicular breath sounds heard
Per abdomen:
Shape of abdomen - obese
Umbilicus - everted
Soft, non tender, bowel sounds heard


CNS:
No focal neurological deficit found
ECG on 5/2/24 ( date of admission)



2d echo







Provisional Diagnosis
? Heart failure
CKD since 3 years


Comments
Post a Comment